

Introduction
Tibial shaft fractures are among the most common long-bone injuries encountered in orthopaedic practice. Intramedullary nailing (IMN) remains the gold standard for definitive management due to its biomechanical stability and minimally invasive nature. Traditionally, the infrapatellar (IP) approach has been widely used; however, the suprapatellar (SP) approach has gained popularity in recent years.
This article provides an academic comparison of suprapatellar and infrapatellar intramedullary nailing techniques, focusing on surgical approach, clinical outcomes, and complications.
Surgical Techniques Overview
Infrapatellar Approach
The infrapatellar approach involves nail insertion with the knee in flexion (typically 90° or more). The entry point is established either through a patellar tendon splitting or medial parapatellar approach.
Key Characteristics:
- Knee in flexed position
- Entry point just below the patella
- Traditional and widely practiced technique
Suprapatellar Approach
The suprapatellar approach is performed with the knee in a semi-extended position using a protective sleeve through the patellofemoral joint.
Key Characteristics:
- Knee in semi-extension (~15–30° flexion)
- Entry via quadriceps tendon above the patella
- Use of cannula to protect intra-articular structures
Biomechanical and Technical Considerations
Fracture Reduction
- SP Approach: Offers superior alignment, particularly in proximal third tibial fractures due to reduced deforming forces.
- IP Approach: Increased difficulty in maintaining reduction, especially in proximal fractures due to quadriceps pull.
Fluoroscopy and Operative Ease
- SP: Easier fluoroscopic imaging due to semi-extended positioning
- IP: Requires repeated manipulation and positioning
Clinical Outcomes
Alignment and Malunion
- Studies show lower malalignment rates with the suprapatellar approach, especially in proximal tibial fractures.
- Infrapatellar nailing has higher rates of valgus and procurvatum deformities.
Postoperative Pain
- Anterior knee pain is more commonly associated with the infrapatellar approach due to patellar tendon violation.
- SP approach demonstrates reduced anterior knee pain, though concerns remain about intra-articular irritation.
Functional Outcomes
- Most studies report comparable long-term functional outcomes between both approaches.
- Early postoperative recovery may favour the suprapatellar technique.
Complications
Infrapatellar Approach
- Anterior knee pain (most common)
- Patellar tendon injury
- Difficulty in proximal fracture fixation
Suprapatellar Approach
- Potential cartilage damage to patellofemoral joint
- Risk of intra-articular contamination (especially in open fractures)
- Learning curve for surgeons
Indications and Preferred Scenarios
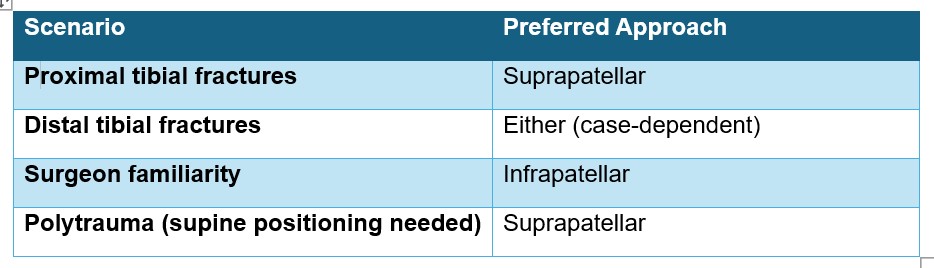
Current Evidence and Literature Trends
Recent meta-analyses and randomized controlled trials suggest that the suprapatellar approach provides better alignment and reduced anterior knee pain, without significant increase in complications when performed correctly. However, long-term data on patellofemoral cartilage health is still evolving.
Conclusion
Both suprapatellar and infrapatellar intramedullary nailing techniques are effective for tibial shaft fractures. The suprapatellar approach offers advantages in terms of alignment, ease of surgery, and reduced anterior knee pain, particularly for proximal fractures. However, concerns regarding intra-articular injury and surgeon familiarity remain.
Ultimately, the choice of approach should be guided by:
- Fracture pattern
- Surgeon expertise
- Available instrumentation
Key Takeaways
- Suprapatellar nailing improves alignment in proximal fractures
- Infrapatellar approach is traditional but associated with more anterior knee pain
- Both techniques yield similar long-term outcomes
- Surgeon experience plays a critical role in success



