
Key Message
- A technically good ACL reconstruction depends on accurate restoration of femoral and tibial insertion anatomy, not only graft choice.
- The ACL is now understood as a broad, ribbon-like and functionally complex structure rather than a simple round cord.
- Non-anatomic tunnel placement can produce persistent pivot shift, graft overload and clinical failure despite a firm Lachman endpoint.
- Modern ACL surgery should be footprint-based, landmark-guided and patient-specific.
Definition and Clinical Importance
The anterior cruciate ligament (ACL) insertion refers to the attachment of the ACL on the medial wall of the lateral femoral condyle and on the anterior intercondylar area of the tibia. Current anatomic reconstruction aims to restore the native ACL footprint, fibre orientation, graft obliquity and rotational control rather than simply placing a graft inside the knee. The femoral and tibial footprints are broad and variable; therefore, tunnel placement should be individualized according to patient anatomy, graft size and associated instability lesions.

From Clock-Face to Footprint: Evolution of Understanding
Earlier ACL teaching was dominated by the two-bundle and clock-face concepts. These remain useful for understanding flexionextension behaviour, but they are insufficient as a sole guide for tunnel placement. Modern studies describe the ACL as a functional continuum with a flat, ribbon-like morphology near the femoral insertion and fan-like expansion toward the tibia. This has shifted surgical thinking from generic tunnel coordinates to patient-specific footprint restoration.

Femoral ACL Insertion: The Critical Zone
The femoral ACL footprint lies on the medial wall of the lateral femoral condyle. It is the most critical area because femoral tunnel position largely determines graft obliquity and rotational stability. Important landmarks are Resident’s ridge, the bifurcate ridge, posterior cartilage margin, ACL remnant fibres and lateral wall morphology. The old clock-face method should be used only as a supportive reference because it does not fully account for knee size, flexion angle or notch morphology.
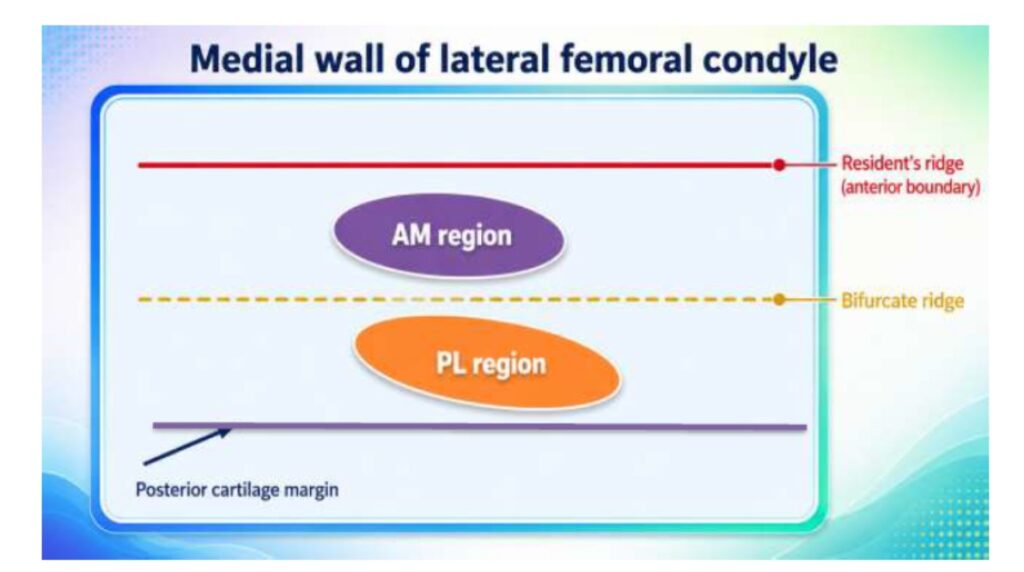

Bifurcate Ridge and AM-PL Functional Regions
The lateral bifurcate ridge separates the anteromedial (AM) and posterolateral (PL) femoral footprint regions. The AM fibres are relatively more important in knee flexion, while PL fibres contribute strongly to extension and rotational control. Although modern anatomy increasingly favours a ribbon-like functional continuum, the AM-PL concept remains clinically useful for tunnel planning,
revision assessment and teaching.

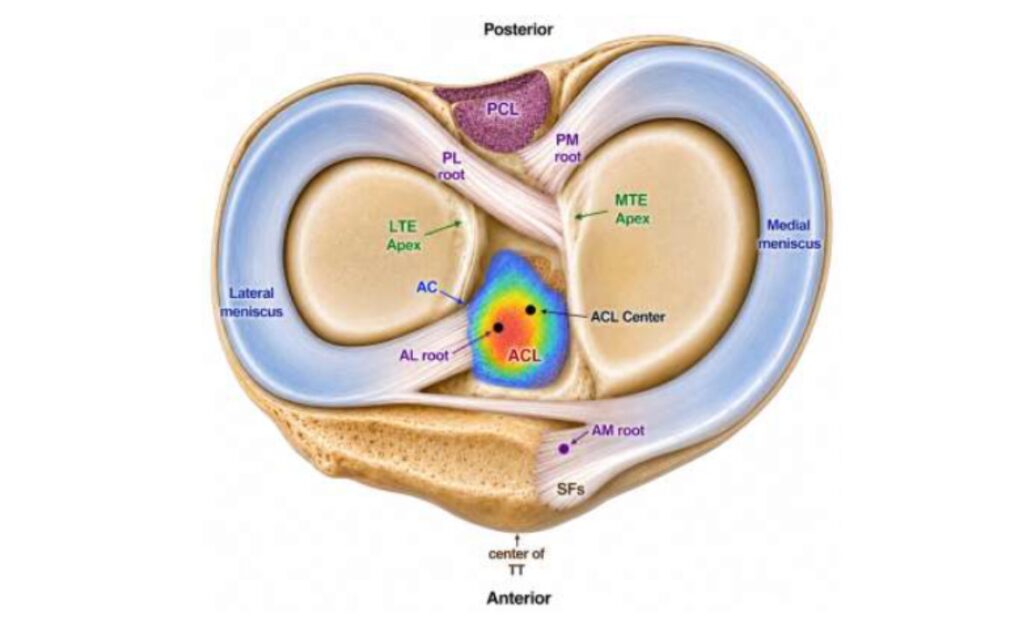
Tibial ACL Insertion: Functional Footprint and Impingement Avoidance
The tibial ACL footprint is located in the anterior intercondylar area of the tibia. It is commonly broader than the prepared graft, meaning that there may be more than one position that appears “anatomic.” The practical target should restore the native line of pull while avoiding anterior notch impingement and excessive posterior placement. Useful tibial landmarks include the ACL remnant, anterior horn of the lateral meniscus, medial tibial spine, intercondylar eminence and relation to the posterior cruciate ligament.
Direct and Indirect Fibers: Why the Footprint Is Not Uniform
The ACL insertion includes direct and indirect fibres. Direct fibres are denser, insert firmly into bone and contribute more to mechanical load transfer. Indirect fibres are fan-like peripheral extensions that broaden the visible footprint. This distinction is important because the visible anatomical footprint may be larger than the true functional graft target. Tunnel placement should therefore restore the functional centre and graft orientation rather than simply occupying any part of the footprint.
Biomechanical Relevance in ACL Reconstruction
An anatomic graft better reproduces the native line of pull of the ACL, improving control of anterior tibial translation and internal tibial rotation. A vertically placed graft may produce a firm endpoint on Lachman testing but may not adequately control pivot shift. Persistent instability after apparently satisfactory ACL reconstruction should trigger evaluation for femoral tunnel malposition, missed ramp lesion, lateral meniscus posterior root tear, anterolateral complex injury, increased posterior tibial slope or generalized laxity.

Single-Bundle, Double-Bundle and Ribbon-Like Reconstruction
Most ACL reconstructions are performed as anatomic single-bundle procedures, aiming to place one graft at the functional centre of the native ACL footprint. Double-bundle reconstruction attempts to separately restore AM and PL bundles, but it is technically more demanding and is usually reserved for selected cases. The ribbon-like ACL concept has encouraged oval or rectangular tunnels, flat graft preparation and remnant-preserving approaches; however, reproducibility, fixation strength and surgeon experience remain essential.
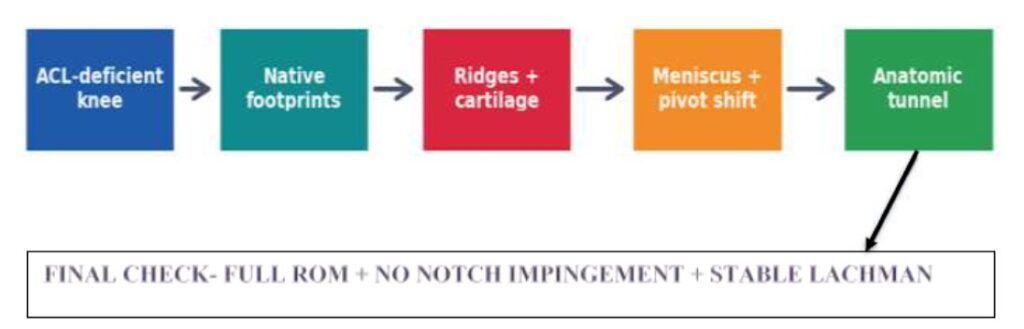
Practical Arthroscopic Checklist

Take-Home Conclusion
Current understanding of ACL insertion has moved from a simplified clock-face model toward a footprint-based, ribbon-like and individualized concept. Successful ACL reconstruction requires accurate femoral and tibial tunnel placement, restoration of graft obliquity, careful interpretation of osseous landmarks and evaluation of associated instability lesions. The modern goal is not merely to reconstruct an ACL, but to restore this patient’s native ACL anatomy and knee biomechanics.