Key academic message: Return to sport after ACL reconstruction should not be cleared on time alone. A safer decision combines biological healing, range of motion, strength symmetry, hop performance, movement quality, knee stability, patient-reported outcomes, and psychological readiness.
Introduction
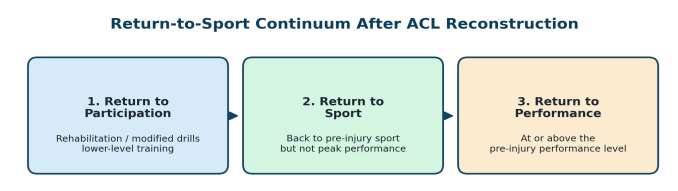
Anterior cruciate ligament reconstruction (ACLR) is commonly performed with the expectation that the patient will return to pre-injury sport. However, return to sport (RTS) is not a single event. It is a graded process in which the patient first resumes rehabilitation and modified training, then returns to the chosen sport, and finally aims to regain pre-injury performance.
A key problem in sports medicine is that RTS cannot be decided safely by calendar time alone. Although graft healing and tissue maturation are important, the athlete must also demonstrate neuromuscular control, adequate strength, landing safety, confidence, and sport-specific readiness. Therefore, RTS should be treated as a clinical decision supported by a structured test battery rather than a routine milestone.
Why Time-Based Clearance Is Incomplete
Many rehabilitation protocols describe approximate timelines, but the same postoperative month can represent very different functional states in two patients. One athlete may have full extension, quiet swelling, good quadriceps control, and confident hopping; another may still have effusion, quadriceps inhibition, poor landing control, or fear of re-injury.
This is why objective and goal-oriented clearance is academically stronger. Time provides context; tests provide evidence. The clinical aim is to identify whether the reconstructed knee can tolerate the demands of acceleration, deceleration, jumping, landing, pivoting, and fatigue.
Phase-Wise Rehabilitation After ACLR
Early phase: protect the knee, restore extension, control swelling
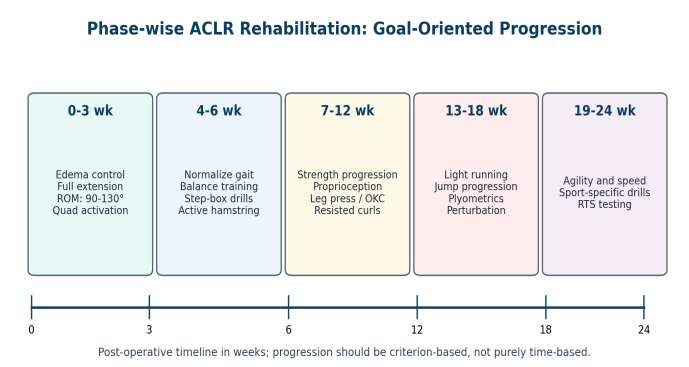
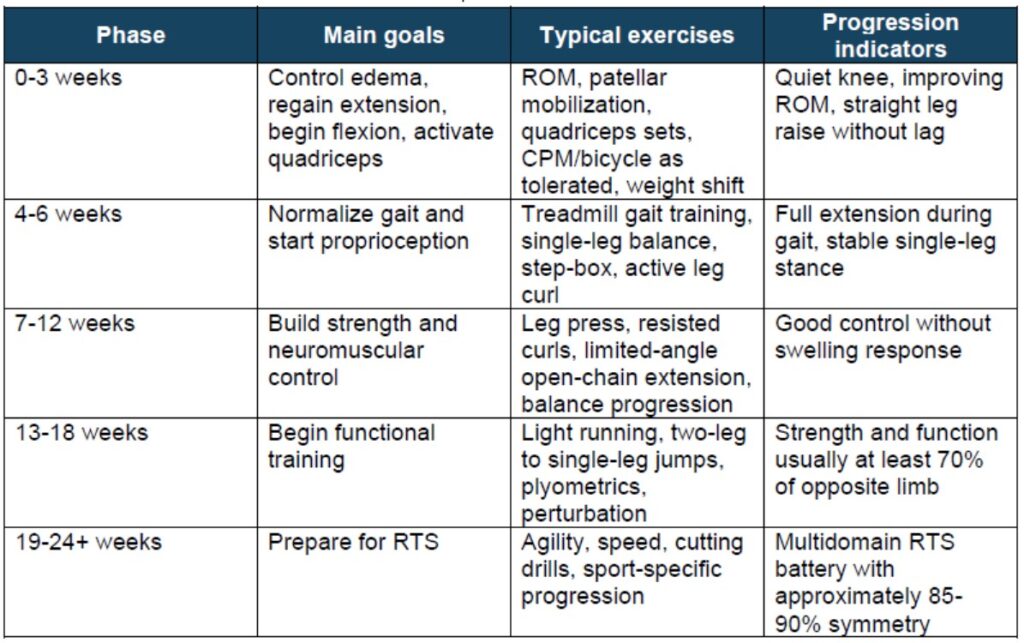
The early phase focuses on inflammation control, restoration of full extension, gradual flexion, quadriceps activation, patellar mobility, and safe weight bearing. Full extension is especially important because extension loss alters gait mechanics and can delay functional recovery.
Intermediate phase: gait, proprioception, and progressive strength
Once pain and swelling are controlled, rehabilitation shifts toward normal walking, single-leg balance, closed kinetic-chain strengthening, step training, and progressive hamstring work. Closed kinetic-chain exercise is useful because it reflects functional loading and encourages cocontraction of the quadriceps and hamstrings.
Advanced phase: running, plyometrics, perturbation, and sport-specific drills
From the later rehabilitation stages, the program should include controlled running, jumping, landing, agility, perturbation training, and graded sport-specific movement. The purpose is not only to make the patient stronger, but also to train feedforward and feedback neuromuscular responses during unexpected movement demands.
Practical Rehabilitation Milestones
Return-to-Sport Assessment: A Test Battery Approach
Patient-reported outcome measures
Patient-reported scores such as IKDC, KOOS, Lysholm, and Tegner activity scale provide insight into symptoms, perceived knee function, sports activity level, and confidence. They should not replace objective tests, but they help interpret whether the athlete feels functionally ready.
Stability and laxity assessment
Clinical assessment includes Lachman, anterior drawer, and pivot shift tests. Instrumented devices such as arthrometers may quantify anterior laxity. Stability testing is important, but it evaluates only part of the problem because many sports injuries occur during dynamic closedchain movement rather than relaxed open-chain examination.
Strength testing
Quadriceps strength is highly relevant after ACLR because quadriceps inhibition and avoidance gait patterns can persist. Hamstring strength is also important, particularly when hamstring autograft is used. Limb symmetry index (LSI) is commonly used, with many protocols expecting approximately 85-90% or higher before unrestricted RTS progression.
Functional performance tests
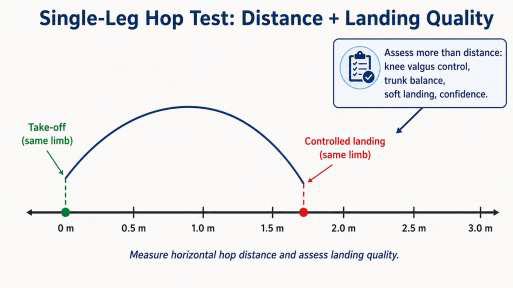
Hop tests assess unilateral power, landing control, confidence, and limb symmetry. Examples include single-leg hop for distance, triple hop, crossover hop, vertical hop, and side hop endurance. However, the clinician should assess both the measured distance and the quality of movement.
Movement quality and balance
Athletes may reach acceptable symmetry on hop distance while still demonstrating poor landing mechanics, dynamic valgus, trunk shift, or poor deceleration control. Movement-quality tools such as landing analysis and balance tools such as the Y-Balance test help identify risk patterns that may be missed by distance-only testing.
Psychological readiness
Fear of re-injury and low confidence are major reasons for delayed or failed RTS, even when physical tests appear satisfactory. Psychological readiness should therefore be part of RTS clearance, especially in pivoting athletes, competitive athletes, and patients with previous graft failure.
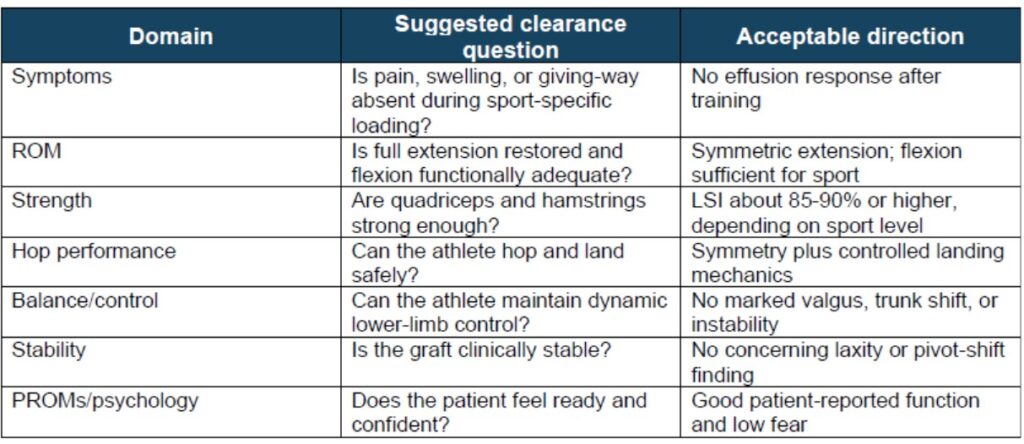
Clinician-Friendly RTS Checklist
Key Take-Home Points
- RTS after ACLR is a continuum: participation, sport, and performance are different milestones.
- Rehabilitation should be progressive and goal-oriented, with early emphasis on extension, edema control, quadriceps activation, and gait normalization.
- Clearance should not be based only on postoperative time; objective functional testing is essential.
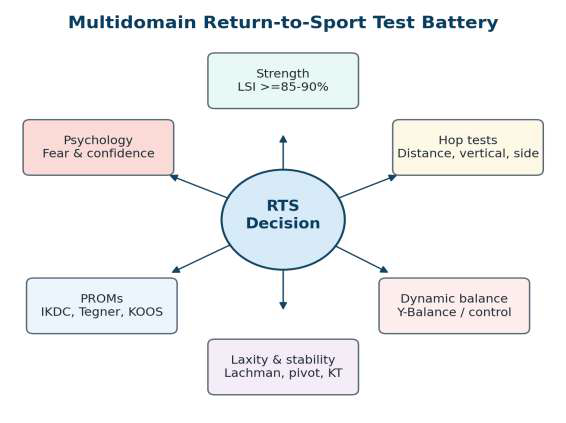
- A strong RTS battery includes strength, hop tests, movement quality, dynamic balance, knee stability, patient-reported function, and psychological readiness.
- Single-leg hop distance is useful, but safe landing mechanics and confidence are equally important.
- Premature return to pivoting sport may increase the risk of graft re-injury or contralateral ACL injury.