
Understanding the Biological and Mechanical Pathways of Bone Repair
Fracture healing is a unique regenerative process in which bone restores its structural integrity without fibrous scar formation. Depending on the mechanical environment and stability at the fracture site, healing proceeds through two distinct but biologically interconnected pathways: primary (direct) fracture healing and secondary (indirect) fracture healing.
Understanding these mechanisms is fundamental for orthopaedic surgeons, as surgical technique and fixation strategy directly influence the healing pathway.
Primary (Direct) Fracture Healing
Primary fracture healing occurs under conditions of absolute mechanical stability, typically achieved through compression plating or lag screw fixation. In this setting, interfragmentary strain is minimal (less than 2%), and there is no visible callus formation.
Biological Mechanism
Primary healing resembles normal bone remodelling and proceeds through:
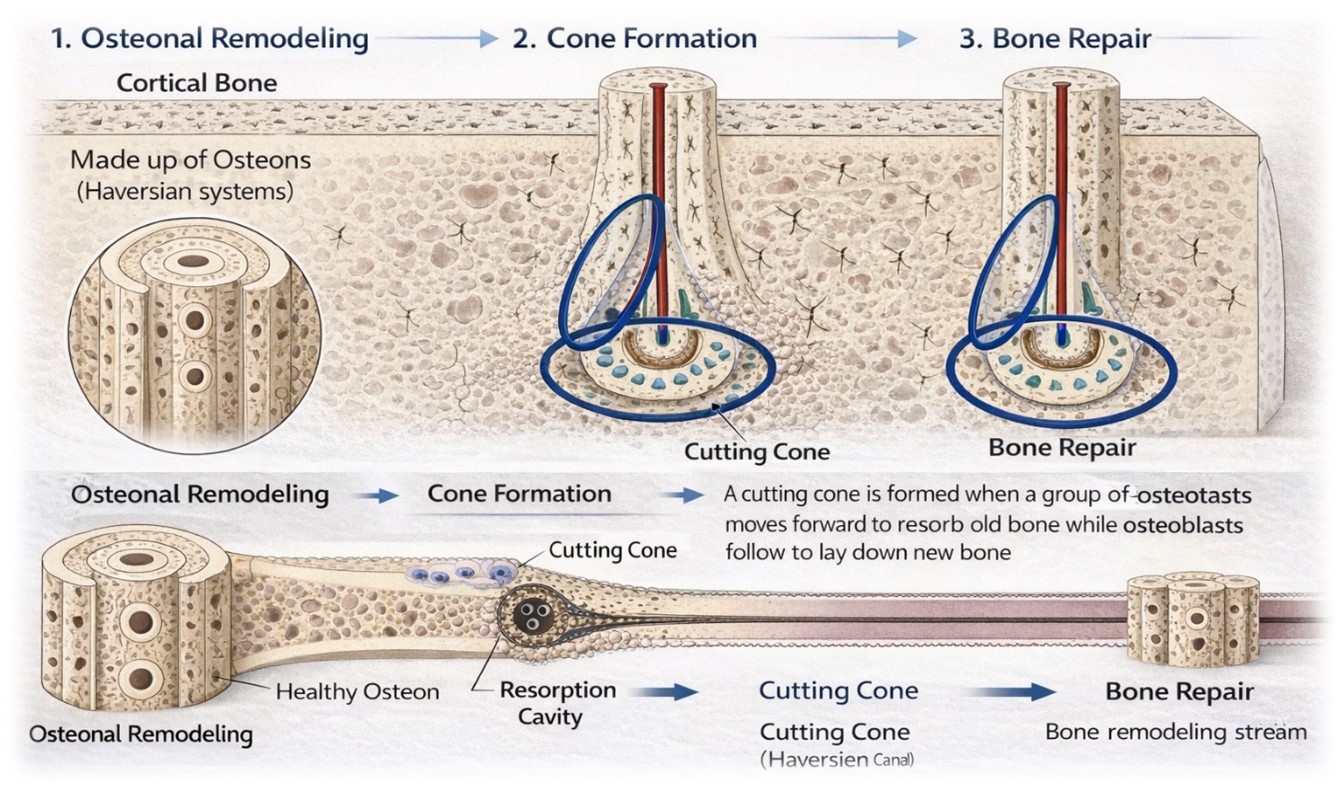
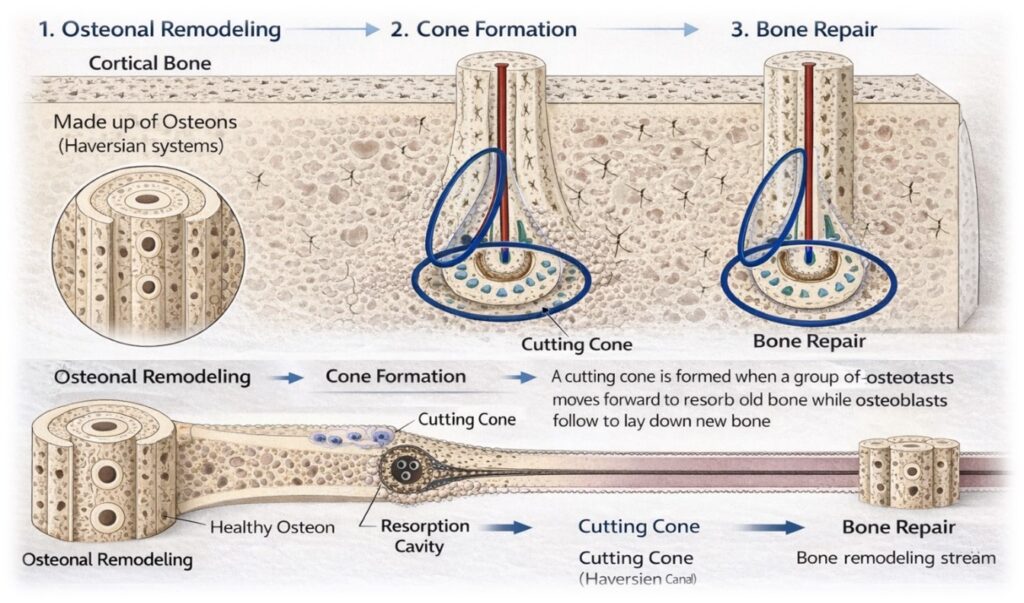
- Contact healing – Occurs when fracture fragments are anatomically reduced with minimal gap (<0.01 mm). Cutting cones composed of osteoclasts cross the fracture line, followed by osteoblast-mediated lamellar bone deposition.
- Gap healing – When a small gap (≤1 mm) exists, woven bone initially fills the space and is subsequently remodelled into lamellar bone through Haversian remodelling.
This process requires:
- Rigid fixation
- Direct cortical contact
- Preserved blood supply
Clinical Applications
Primary healing is commonly observed in:
- Compression plating of long bone fractures
- Intra-articular fractures requiring anatomical reduction
- Elective osteotomies
The advantage of this pathway is precise anatomical restoration; however, it demands meticulous surgical technique and stable fixation.
Secondary (Indirect) Fracture Healing
Secondary fracture healing is the more common biological pathway and occurs under conditions of relative stability, such as bridge plating, intramedullary nailing, or cast immobilization.
Unlike primary healing, this process involves callus formation and progresses through distinct biological stages.
Phases of Secondary Healing
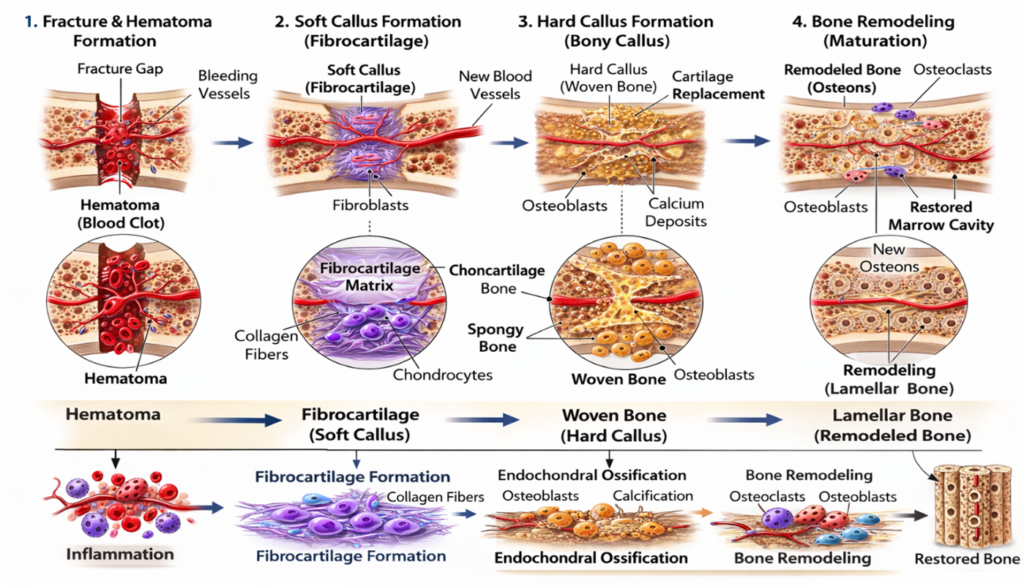
Inflammatory Phase
Hematoma formation occurs immediately after fracture, accompanied by inflammatory cytokine release and recruitment of mesenchymal stem cells.
Reparative Phase
Formation of soft callus (fibrocartilage)
Conversion to hard callus (woven bone) through endochondral ossification
Remodelling Phase
Woven bone is gradually replaced by lamellar bone, restoring mechanical strength and architecture.
Secondary healing tolerates controlled micromotion, which stimulates callus formation. However, excessive instability may lead to delayed union or non-union.
Clinical Applications
Secondary healing is seen in:
- Intramedullary nailing
- External fixation
- Conservative management with casting
- Bridge plating techniques
This pathway is biologically robust and often preferred in comminuted fractures where anatomical compression is not feasible.
Table 1: Describes key Differences Between Primary and Secondary Healing
| Feature | Primary Healing | Secondary Healing |
| Stability | Absolute | Relative |
| Interfragmentary strain | <2% | 2–10% |
| Callus formation | Absent | Present |
| Type of ossification | Intramembranous | Endochondral |
| Typical fixation | Compression plate | IM nail, bridge plate, cast |
Mechanical Environment and Strain Theory
The concept of interfragmentary strain, described by Perren, explains how the mechanical environment determines tissue differentiation. High strain Favors fibrous tissue, moderate strain promotes cartilage formation, and low strain supports bone formation. Thus, fixation strategy directly dictates the healing pathway.
Clinical Implications
- Absolute stability is essential for articular fractures to prevent post-traumatic arthritis.
- Relative stability is advantageous in comminuted fractures to preserve biology.
- Preservation of periosteal blood supply is critical in both pathways.
- Overly rigid constructs in comminuted fractures may impair callus formation.
Modern fracture management increasingly balances mechanical optimization with biological preservation, aligning with broader concepts such as biological fixation and the Diamond Concept.
Conclusion
Primary and secondary fracture healing represent two biologically distinct responses determined by mechanical stability. While primary healing requires rigid fixation and anatomical reduction, secondary healing leverages controlled micromotion and callus formation to achieve union.
Successful fracture management requires understanding these pathways and selecting fixation strategies that optimize both mechanical and biological conditions.