As soon as a trauma surgeon looks at an X-ray of a fracture, a whole maze of decisions starts to float in his head. What kind of fixation construct will the bone heal fastest with? Is there any special patient factor that requires changes in the treatment plan? How can the characteristics of the implants be compatible with the quality of the bone, the condition of the soft tissue and the overall health of the patient?
From high-energy traffic accidents to the fragile bones of elderly people, trauma incidents always require a lot of technical skills plus a very well thought-out surgical decision, making approaches based on clinical best practices. The implant choice, fracture type, the patient’s other diseases, and the patient’s biological healing potential all influence the treatment outcome.
The Foundation: Evidence-Based Decision Frameworks
The Four Cs of Surgery have been and will remain the basics of surgery: precise restoration of anatomy, stable fixation, minimal trauma with preservation of blood supply to tissues and early mobilization. However, their usage may be different depending on the nature of the fracture. A simple transverse fracture of long bones of the legs or arms can be made absolutely stable by means of a compression plate or a locked intramedullary nail. The comminuted metaphyseal fractured bones may be given relative stability by using a bridge plating technique that helps in maintaining the alignment while the bone is healed secondarily.
The decision about the exact kind of implant basically hinges on this one thing. The regular dynamic compression plates are good at putting pressure on a certain area of the bone to close the gap and thus help in healing. On the other hand, the locking plate systems may be necessary when stabilizing by angular means, which must be obtained from the plate, screw assembly itself. Knowing when each mechanical environment is optimal for healing, and which implant features allow that environment, is the difference in surgical decision-making between the competent and the very best ones.
Before choosing an implant, surgeons evaluate several core parameters:
- Fracture type and classification
- Soft tissue condition
- Bone quality
- Patient age and activity level
- Presence of comorbidities (diabetes, smoking, osteoporosis)
- Surgeon expertise and institutional protocols
The Implant Selection Decision Tree: A Systematic Approach
Once trauma surgeons gain experience, they can embed into their minds decisions, making algorithms that help them quickly and effectively limit the kind of implants they might use. Such mental structures lead them step by step through a series of filters:
Basic (first-order) factors are what basically determine the main category of fixation. Can this fracture be treated with an intramedullary nail? Does the extension of the periarticular area require the use of a plate? Could an external fixation device serve both the mechanical and biological needs?
Second order refinements concentrate on the implant details. In the case of plates, should they be locking or conventional? Anatomically pre-contoured or a simple generic reconstruction plate? For nails: should they be reamed or unreamed? What locking variations correspond to the fracture location?
Third–order adjustments refer to particular features of systems. Is this locking plate one that would provide polyaxial screw options? Is it possible to use combination holes? Does the set of instruments include sufficient tools for reduction?
Best Practices for Implant Selection in Orthopedic Trauma Surgery
Implant selection directly impacts mechanical stability, biological healing, and long-term functional outcomes.
1. Match Implant to Fracture Pattern
Different fracture configurations require different mechanical solutions:
- Transverse fractures → Compression plating
- Comminuted fractures → Bridging plates or intramedullary nails
- Intra-articular fractures → Anatomically contoured plates
- Long bone diaphyseal fractures → Intramedullary nails
A mismatch between implant design and fracture mechanics can lead to non-union, implant failure, or malalignment.
2. Respect Biological Fixation
Overly rigid constructs can impair callus formation. Locking plates, for example, function as internal fixators and reduce periosteal disruption when applied properly.
Surgeons must balance absolute stability (primary bone healing) and relative stability (secondary bone healing).
3. Consider Soft Tissue Envelope
In high-energy trauma, preserving soft tissue is paramount.
- Minimal invasive plating techniques (MIPPO)
- Percutaneous intramedullary nailing
- Temporary external fixation in damage control orthopedics
Implant choice should complement soft tissue management, not compromise it.
The Critical Role of Implant Stability in Bone Healing
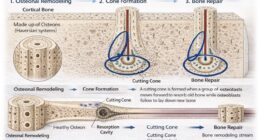
Fracture healing goes on with phases overlapping. The first is inflammation, next soft callus formation, hard callus formation, and finally remodeling and each necessitates its own mechanical environment. It is known that severe motion at the fracture site will interfere with the biological cascade. Overgenerously, too much motion leads to the formation of fibrous tissue instead of bone formation. On the other hand, absolute stability means that fracture site motion is totally eliminated, thus permitting primary bone healing. Relative stability, in contrast, allows controlled micromotion that, in turn, stimulates secondary healing through callus formation.
Implant selection should be such that the mechanical environment matches the healing pathway. Compression plating realizes absolute stability and, therefore, is a good choice for simple fracture patterns where anatomic reduction restores cortical continuity. Bridge plating, which provides relative stability, is thus the way to treat comminuted fractures. Intramedullary nails give off load to the bones rather than bear the load, which is perfect for diaphyseal fractures.
The biomechanical principles are there, but their implementation depends on implants with performance characteristics that can be predicted. Locking screws have to be able to maintain angular stability through cyclic loading. The materials used for the plates have to be capable of balancing rigidity with flexibility that will not result in stress shielding.
Manufacturing accuracy must guarantee that the designed mechanical properties are always clinically effective. These quality necessities are the reasons GPC Medical Ltd. is committed to quality management systems. In fact, ISO 13485 certification is a token of that commitment to providing performance consistency upon which surgeons base their trust.
How GPC Medical Ltd. Supports Clinical Excellence?
Increasingly, surgeon feedback and clinical data guide implant innovation. A surgeon-centric approach to product design – one that listens to real clinical challenges and iterates accordingly – has become a hallmark of advanced orthopedic solutions. Leading implant manufacturers like GPC Medical Ltd. exemplify this philosophy by investing in quality, technology, and manufacturing excellence to support clinical best practices.
Quality and manufacturing precision are not optional in trauma implants – they are essential.
GPC Medical Ltd. employs:
- Advanced manufacturing technologies
- High-precision machining
- Biocompatible materials and stringent quality controls
- Process standardization aligned with international regulatory standards
These systems ensure implants possess:
- High fatigue resistance
- Reliable locking mechanisms
- Accurate dimensional consistency
- Excellent surface finish for bone conformity
Coupled with surgeon-driven design, these manufacturing strengths translate into implants that fit better, perform predictably, and support clinical best practices.
GPC Medical’s commitment to quality also extends to education – offering surgical technique guides, hands-on workshops, and digital resources that help surgeons make informed decisions for optimized patient outcomes.